Free Nys 100 Form
Free Nys 100 Form
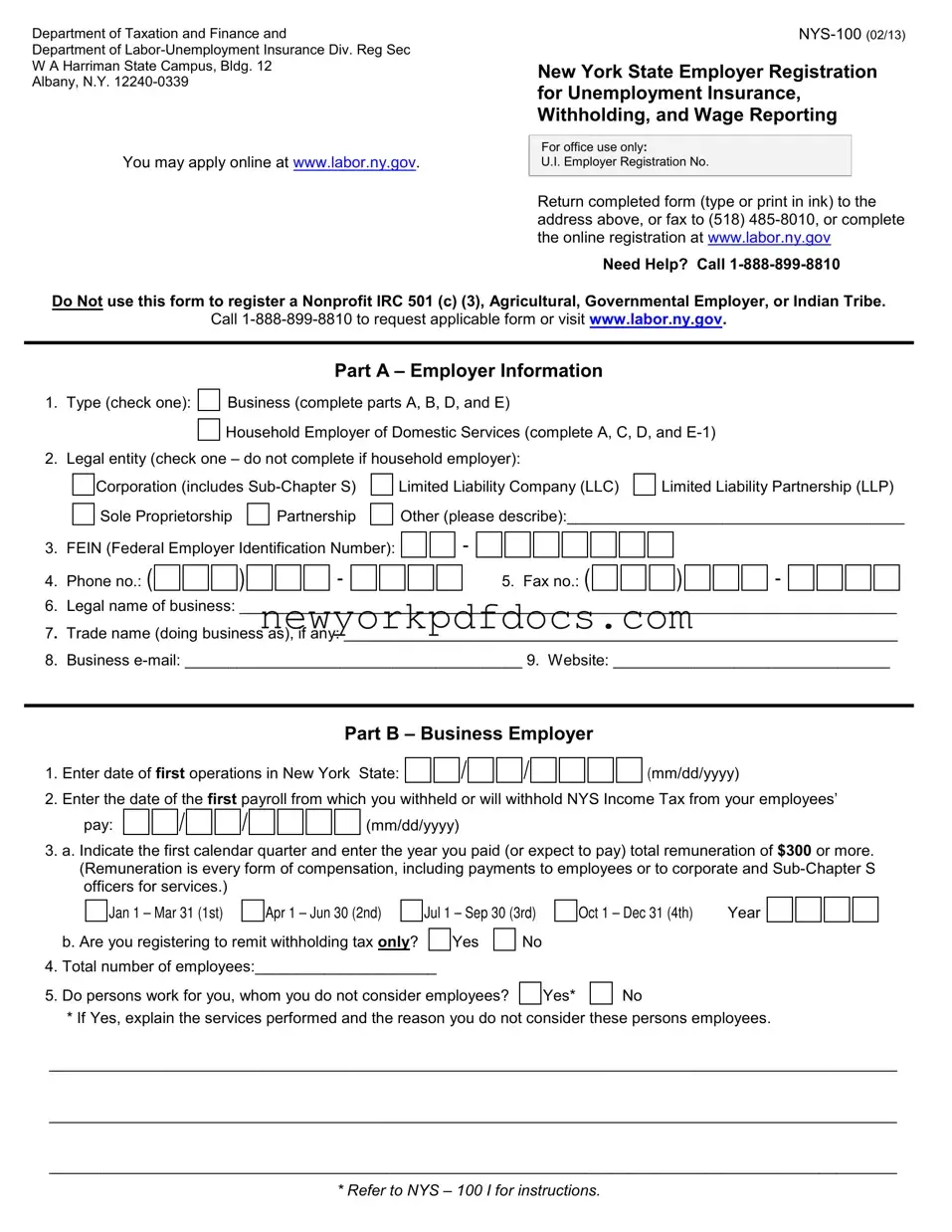
The NYS-100 form is an essential document for employers in New York State, designed to facilitate the registration process for unemployment insurance, withholding tax, and wage reporting. This form is particularly important for businesses and household employers alike, as it ensures compliance with state regulations. When filling out the NYS-100, employers must provide detailed information about their business structure, including whether they operate as a corporation, partnership, or sole proprietorship. Additionally, the form requires employers to disclose their Federal Employer Identification Number (FEIN), contact information, and the date they began operations in New York. For household employers, there are specific sections to report domestic services and the total cash wages paid. Furthermore, the NYS-100 includes requirements for addresses, ensuring that the appropriate tax correspondence reaches the right location. Employers should be aware that this form is not applicable for certain entities, such as nonprofit organizations or governmental employers, and they must seek alternative registration forms if needed. Overall, understanding the components of the NYS-100 is crucial for any employer looking to operate within New York State legally and efficiently.
IRS Form SS-4: This form is used to apply for an Employer Identification Number (EIN). Like the NYS-100, it collects essential information about the business structure and ownership, which is crucial for tax purposes.
IRS Form W-2: Employers use this form to report wages paid to employees and the taxes withheld. Similar to the NYS-100, it is essential for compliance with tax regulations and employee wage reporting.
IRS Form 941: This quarterly form reports income taxes, Social Security tax, and Medicare tax withheld from employee paychecks. It parallels the NYS-100 in its focus on employee compensation and tax obligations.
New York State Form IT-2104: This form allows employees to determine the amount of state income tax withholding. Like the NYS-100, it is related to tax withholding but is focused on employee rather than employer information.
New York State Form NYS-45: This quarterly report summarizes wages paid and taxes withheld for unemployment insurance. It serves a similar purpose as the NYS-100 in reporting employee-related information to the state.
IRS Form 1099-MISC: Used to report payments made to independent contractors. Like the NYS-100, it helps ensure that all compensation is reported for tax purposes, though it focuses on non-employee compensation.
New York State Form DTF-95: This form is for businesses to register for sales tax. It is similar to the NYS-100 in that it is a registration form, but it focuses on sales tax obligations rather than unemployment insurance.
New York State Form NYS-1: This form is used to report and pay withholding tax. It parallels the NYS-100 in its focus on employer tax responsibilities related to employee wages.
IRS Form 940: Employers use this annual form to report their Federal Unemployment Tax Act (FUTA) tax. Like the NYS-100, it is concerned with unemployment taxes but at the federal level.
New York State Form CT-1: This form is for corporations to report their annual franchise tax. Similar to the NYS-100, it involves compliance with state tax regulations, although it targets corporate entities specifically.
Department of Taxation and Finance and
Department of
Albany, N.Y.
New York State Employer Registration for Unemployment Insurance, Withholding, and Wage Reporting
You may apply online at www.labor.ny.gov.
For office use only:
U.I. Employer Registration No.
Return completed form (type or print in ink) to the address above, or fax to (518)
Need Help? Call
Do Not use this form to register a Nonprofit IRC 501 (c) (3), Agricultural, Governmental Employer, or Indian Tribe.
Call
Part A – Employer Information
1. |
Type (check one): |
|
Business (complete parts A, B, D, and E) |
|
|
|||||||
|
|
|
|
|
Household Employer of Domestic Services (complete A, C, D, and |
|||||||
|
|
|
|
|
||||||||
2. |
Legal entity (check one – do not complete if household employer): |
|
|
|||||||||
|
|
|
Corporation (includes |
|
Limited Liability Company (LLC) |
|
Limited Liability Partnership (LLP) |
|||||
|
|
|
|
|
||||||||
|
|
|
Sole Proprietorship |
|
Partnership |
|
|
Other (please describe):_______________________________________ |
||||
|
|
|
|
|
|
|||||||
3. FEIN (Federal Employer Identification Number):
-
4. Phone no.: ( |
|
|
|
|
|
) |
|
|
|
|
|
- |
|
|
|
|
|
|
|
5. Fax no.: ( |
|
|
|
|
|
) |
|
|
|
|
|
- |
6.Legal name of business: ____________________________________________________________________________
7.Trade name (doing business as), if any: ________________________________________________________________
8.Business
Part B – Business Employer
1. |
Enter date of first operations in New York |
State: |
|
|
|
/ |
|
|
|
/ |
|
|
|
|
|
|
|
(mm/dd/yyyy) |
|||||||||||||||
2. |
Enter the date of the first payroll from which you withheld or will withhold NYS Income Tax from your employees’ |
||||||||||||||||||||||||||||||||
|
pay: |
|
|
|
/ |
|
|
|
/ |
|
|
|
|
|
|
|
(mm/dd/yyyy) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
3.a. Indicate the first calendar quarter and enter the year you paid (or expect to pay) total remuneration of $300 or more. (Remuneration is every form of compensation, including payments to employees or to corporate and
|
|
|
Jan 1 – Mar 31 (1st) |
|
Apr 1 – Jun 30 (2nd) |
|
Jul 1 – Sep 30 (3rd) |
|
Oct 1 – Dec 31 (4th) |
Year |
||||||||
|
b. Are you registering to remit withholding tax only? |
|
|
Yes |
|
|
No |
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
||||||||||
4. |
Total number of employees:_____________________ |
|
|
|
|
|
|
|
|
|||||||||
5. |
Do persons work for you, whom you do not consider employees? |
|
|
Yes* |
|
|
No |
|
||||||||||
|
|
|
|
|
||||||||||||||
*If Yes, explain the services performed and the reason you do not consider these persons employees.
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
* REFER TO NYS – 100 I FOR INSTRUCTIONS.
NYS 100 page 2 |
|
|
|
|
|
Legal Name: __________________________________ER Number: _________________________ |
|||||||||||||||||||||||||||||||||||||||||||||||
6. |
Have you acquired the business of another employer liable for NYS Unemployment Insurance? |
|
|
|
|
|
Yes* |
|
No |
||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||||
|
* If Yes, did you acquire |
|
All or |
|
|
Part? |
Date of acquisition: |
|
|
|
|
|
/ |
|
|
|
/ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(mm/dd/yyyy) |
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||
|
Prior Owner’s: Registration number: |
|
|
|
|
- |
|
|
|
|
|
|
|
|
|
|
|
FEIN: |
|
|
|
- |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
Legal name of business: ______________________________________________________________ |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Address:___________________________________________________________________________ |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
7. |
Have you changed legal entity? |
|
|
Yes* |
|
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
* If Yes, date of legal entity change: 

 Previous employer’s: Registration number:
Previous employer’s: Registration number:
/
/
-
(mm/dd/yyyy)
FEIN:
-
Part C – Household Employer of Domestic Services
1. Indicate the first calendar quarter and enter the year you paid (or expect to pay) total cash wages of $500 or more:
|
|
|
Jan 1 – Mar 31 (1st) |
|
Apr 1 – Jun 30 (2nd) |
|
Jul 1 – Sep 30 (3rd) |
|
|
Oct 1 – Dec 31 (4th) |
Year |
|||
2. |
Enter the total number of persons employed in your home: ________________________ |
|
||||||||||||
|
|
|
|
|
|
|
|
|||||||
3. |
Will you withhold New York State income tax from these employees? |
|
|
Yes |
|
No |
|
|||||||
Part D – Required Addresses
1.Mailing Address: This is your business mailing address where your Withholding Tax (WT) and Unemployment Insurance (UI) mail will be delivered. However, if you elect to have your UI mail directed to an address other than your place of business, complete number 4 below.
Street or PO Box: _______________________________________________________________________________
City:_______________________________________________________ State: _________ZIP Code:____________
2.Physical Address: This is the physical location of your business, if different from the Mailing Address in number 1.
Street: ________________________________________________________________________________________
City:_______________________________________________________ State: _________ZIP Code:____________
3.Location of Books/Records: This is the physical location where your Books and Records are maintained.
Street: ________________________________________________________________________________________
City:_______________________________________________________ State: _________ZIP Code:____________
Optional Addresses
4.Agent Address (C/O): Complete this if your UI mail should be sent to an address other than your business address.
C/O: __________________________________________________________________________________________
Street or PO Box: _______________________________________________________________________________
City:_______________________________________________________ State: _________ZIP Code:____________
Telephone: (
)
-
ext:________________
5.LO 400 Form - Notice of Entitlement and Potential Charges Address: If completed, this is where the LO 400 will be directed. (It is mailed each time a former employee files a claim for Unemployment Insurance benefits.)
C/O: __________________________________________________________________________________________
Street or PO Box: _______________________________________________________________________________
City:_______________________________________________________ State: _________ZIP Code:____________
Telephone: (
)
-
ext:________________
* REFER TO NYS – 100 I FOR INSTRUCTIONS.
NYS 100 page 3 |
Legal Name: __________________________________ER Number: _________________________ |
Part E – Business Information
1.Complete the following for sole proprietor (owner), household employer of domestic services, all partners, including partners of LP, LLP or RLLP, all members of LLC or PLLC, and corporate officers (President, Vice President, etc.), whether or not remuneration is received or services are performed in New York State.
Name |
|
Social Security |
|
Title |
|
Residence Address |
|
|
Number |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2.Please enter the number of physical locations at which your company operates: _____. You MUST list the physical address and answer questions A through E below, for each location. Use a separate sheet of paper for each.
a. Location: _______________________ |
____________________ |
_____________________ |
___________ |
Number and Street |
City or Town |
County |
Zip Code |
b. Approximately how many persons do you employ there? _______________
c. Check the principal activity at the above location:
Manufacturing
Wholesale trade
Retail trade
Construction
Warehousing
Transportation
Computer services
Educational services
Health & social assistance
Real estate
Scientific/professional & technical services
Finance & insurance
Arts, entertainment & recreation
Food service, drinking & accommodations
Corporate, subsidiary managing office
Other (Please specify):_____________________________________________________________________
d. If you are primarily engaged in manufacturing, complete the following:
Principal Products Produced |
Percent of Total Sales Value |
Principal Raw Materials Used |
____________________________ |
__________________________ |
_________________________ |
e. If your principal activity is not manufacturing, indicate products sold or services rendered:
Type of Establishment |
Principal Product Sold or |
Percent of Total Revenue |
|
Service Rendered |
|
_____________________________ |
__________________________ |
________________________ |
I affirm that I have read the above questions and that the answers provided are true to the best of
my knowledge and belief.
X________________________________________________________________
Signature of Officer, Partner, Proprietor, Member or Individual
_______________________________________________ Phone no.: (
Official Position
)
|
/ |
|
|
|
/ |
|
(mm/dd/yyyy)
-
* REFER TO NYS – 100 I FOR INSTRUCTIONS.
Completing the NYS-100 form accurately is crucial for employers registering for unemployment insurance, withholding, and wage reporting in New York State. However, several common mistakes can hinder the registration process. Understanding these pitfalls can help ensure a smoother submission.
One frequent error is failing to provide the correct Federal Employer Identification Number (FEIN). This number is essential for identification and tax purposes. Omitting or incorrectly entering this number can lead to delays in processing the application. Employers should double-check this information before submission.
Another mistake involves not selecting the appropriate type of employer at the beginning of the form. Employers must indicate whether they are a business or a household employer. Choosing the wrong category can result in incomplete sections being filled out, leading to potential rejections or requests for additional information.
Many applicants also overlook the importance of providing accurate contact information. This includes phone numbers and email addresses. Missing or incorrect contact details can hinder communication from the Department of Labor, which may require follow-up information or clarification on the application.
In Part B, employers often miscalculate the total number of employees. Underreporting or overreporting can cause discrepancies in tax obligations. It is crucial to provide an accurate count of employees to ensure compliance with state regulations.
Some individuals fail to specify if they have acquired the business of another employer. This section is vital for determining liability for unemployment insurance. Neglecting to answer this question can lead to complications in the registration process.
Furthermore, applicants sometimes forget to provide required addresses. The mailing address, physical address, and location of books and records must be clearly stated. Incomplete address information can delay the processing of tax documents and notifications.
Another common oversight is failing to sign the form. The signature of an authorized individual is necessary to validate the application. Without a signature, the form may be deemed incomplete and returned.
Lastly, individuals may neglect to review the instructions provided with the NYS-100 form. These instructions contain critical information that can guide applicants through the process and help avoid common pitfalls. Taking the time to read the instructions can lead to a more efficient registration experience.
The NYS-100 form, officially known as the New York State Employer Registration for Unemployment Insurance, Withholding, and Wage Reporting, is a document that businesses must complete to register for unemployment insurance and withholding taxes in New York State. This form is essential for employers who hire employees and need to comply with state tax regulations.
Any business or household employer that hires employees in New York State is required to complete the NYS-100 form. This includes corporations, limited liability companies (LLCs), sole proprietorships, and partnerships. However, nonprofit organizations, agricultural employers, governmental employers, and Indian tribes should not use this form. Instead, they should contact the Department of Labor for the appropriate registration form.
You can submit the NYS-100 form in several ways. You may apply online at www.labor.ny.gov. Alternatively, you can print the completed form and mail it to the address provided on the form, or fax it to (518) 485-8010. Make sure to complete the form accurately to avoid any delays in processing.
The NYS-100 form requires various pieces of information. You will need to provide details about your business, such as the legal name, trade name, and contact information. Additionally, you must indicate the type of business entity, date of first operations in New York, and the total number of employees. If you are a household employer, specific details about your domestic employees will also be needed.
If you have questions or need assistance while completing the NYS-100 form, you can call the New York State Department of Labor at 1-888-899-8810. They can provide guidance and help clarify any uncertainties you may have about the registration process.
Once you submit the NYS-100 form, the Department of Labor will process your registration. If everything is in order, you will receive a U.I. Employer Registration Number, which you will need for future tax filings and compliance. Keep this number in a safe place, as it will be important for your business operations.
Here are five common misconceptions about the NYS 100 form, which is used for employer registration for unemployment insurance, withholding, and wage reporting in New York State.
Dmv Plate Drop Off - Keep in mind that your surrender application is not effective until processed by DMV.
Articles of Amendment Llc - The Certificate of Amendment is used to officially change the details of a corporation's certificate of incorporation in New York.
Filling out the NYS-100 form is a crucial step for employers in New York State. This form is used for registering for Unemployment Insurance, withholding taxes, and wage reporting. Here are some key takeaways to keep in mind:
These points highlight the importance of accuracy and completeness when filling out the NYS-100 form. Following these guidelines will help ensure a smoother registration process and compliance with state regulations.
Filling out the NYS-100 form is an essential step for employers in New York State to register for unemployment insurance, withholding, and wage reporting. Completing this form accurately ensures compliance with state regulations and facilitates proper tax management. Below are the steps to guide you through the process.